
INTRODUCTION
The essence of
antenatal care is a thorough assessment at the first visit (history,
examination, routine and indicated investigation) followed by assessments
thereafter at appropriate intervals. This will reveal existing risk factors and
any further deviations from normal at the earliest opportunity.
Risk factor analysis
can be a complex and time consuming procedure since it may involve a wide range
of factors. Major emphasis is placed on the preventive aspects of care – education
and motivation of the woman, immediate medical care, referral for investigation
or expert opinion, or an increase in the tempo of surveillance.
Proper antenatal
management involves seeing the woman as early as practicable in the pregnancy, considerable
care in obtaining all relevant information about the woman by history taking,
examination and special investigation, thinking carefully about its obstetric
significance and taking appropriate corrective action.
The meaning of the
pregnancy to the mother and partner should be ascertained in terms of
acceptance, preparedness and coping ability, any major stress, financial or
other, should be determined. An overriding consideration of antenatal care is
detection of the risk factors for both mother and baby, and reducing these to
manageable and safe proportion by further investigation as indicated and
matching risk to appropriate level.
In extreme case,
this may involve the antenatal diagnosis of major foetal anomaly and
termination of the pregnancy if thought to be necessary. The antenatal period
is the ideal time to provide the mother with appropriate health education. E.g.
diet, rest, exercise, breast feeding; the potential harm to the baby from alcohol
and smoking should be indicated.
Antenatal care is a
planned programmed of observation, education, and medical management of pregnant
woman directed towards making pregnancy and delivery a safe and satisfying
experience.
Women should attend
ANC monthly up to 28 weeks then 2 weeks up to 36 weeks and then weekly 36 weeks
thereafter.
High risk Mothers
e.g. multiple pregnancies, suspected disproportion etc. should attend weekly.
THE FIRST VISIT:
this is the particular routine through which the woman passes, it depends on variables
such as private or public care and the size of the institution in the latter
case.
INFORMATION TO OBTAIN DURING THE FIRST
VISIT/ASSESSMENT
HISTORY
this
involves taking information about the pregnant woman for the first time. The
information should include:
- ADMINISTRATIVE DETAILS:
these include the woman’s particulars such as name, place of abode, date of
birth, occupation, next of kin, religion etc.
- FAMILY HISTORY:
condition likely to be inherited by the woman such as diabetes, hypertension.
Psychiatric disorders, twins, haemoglobinopathy etc.
- MEDICAL HISTORY:
any of the following should be noted; allergies, cardiac disease, hypertension,
renal diseases, central nervous disorders, psychoses, gastrointestinal or metabolic
disease, blood transfusions rubella; any medications should be recorded.
- SURGICAL HISTORY:
abdominal or pelvic operations in particular, as well as cardiac surgery and also
injuries are recorded.
- SOCIAL HISTORY:
relevant socioeconomic data are obtained, including information on the family
adjustment and living conditions, and unusual stresses. Consumption of alcohol
and drugs of addiction should be determined.
- GYNECOLOGICAL HISTORY: a history of venereal disease is important. Also previous disorders,
such as abnormal cytology, infertility and gynecological surgery, are relevant.
- OBSTETRIC HISTORY:
accurate details of all previous pregnancies must be obtained, including the
year, period of gestation, duration of labour, nature of delivery and outcome,
including sex and weight of the baby; also complication arising during
pregnancy, labour and puerperium.
- PRESENT HISTORY:
the history of the present pregnancy is obtained, which includes a careful
review of all the systems. The date of last menstrual period should be noted,
any contraceptive pill used, any infection she suffered; the woman diet during
the pregnancy should be assessed etc.
SIGNIFICANCE/REASONS FOR ANTENATAL CARE
- To assist pregnant
women to meet the nutritional status appropriate to their state.
- To identify any
complication and find solution to it or to issue appropriate referrals.
- To educate them on
public health issues such as malaria, hand washing after visiting the toilet,
etc.
- To teach the women
about labour, labour pains and what is expected during the labour process.
- To share
information about what pregnancy is, how the baby grows and the need to take medication
given at the antenatal care.
- To facilitate the
woman and the family in preparation toward delivery.
SERVICES RENDERED AT THE ANTENATAL CARE
- Offering family
planning services to couples and individual who need them.
- Provision of
immunization to children.
- Offering counseling
service to people.
- Rendering under
five (5) clinics to mothers and their children.
- Treatment of minor
ailment.
- Laboratory
Investigations.
- Screening and
treatment of STI.
GENERAL EXAMINATION
Three (3) techniques
are employed here to examine the pregnant woman at the antenatal clinic. The examinations
are carried out from head to toe of the woman. While going through the
examination, you take note of any abnormalities that you may notice, so that
appropriate measures can be put in place. The aspects considered include;
Inspection: This
involves looking at the woman from the head to toe.
Her appearance
observe
the way she walk, any rashes on her body. Observe the breast for any abnormal
changes. Observe the vaginal for any soreness, warts and discharges. Observe
the mouth for sore, scent, swelling etc. Observe the extremities for edema
which may suggest PIH, any varicose veins on the legs, watch the colour of the
nails. Watch the abdomen to see whether it is pendulous or not. As it may give
clue that the woman may have contracted pelvis.
Palpation
this is
done on the abdomen. You palpate the abdomen to know the gestation age, the position
of the baby, any stretch marks on the abdomen, the fundal height, movement of
the foetus and the presentation.
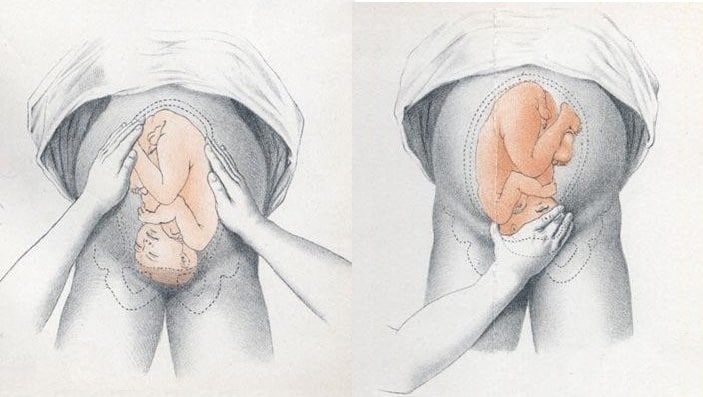 |
Photo by teachmeobgyn.com
|
Auscultation
the
foetal heart becomes audible with the clinical Doppler instrument at about 12 weeks
gestation and stethoscope auscultation at about 18-20 weeks. But mostly at our
ANC they use fetoscope to hear the heart sound of the foetus.
 |
Photo by 123rf.com
|
PROCEDURE TO FOLLOW WHEN CONDUCTING
ANTENATAL EXAMINATION
- First and for most,
provide privacy and give reassurance to your client.
- Before examination,
ask the woman to empty her bladder.
- Quickly inspect the
woman from head to toe. Starting from the head, look at the colour of the hair.
Look at the conjunctiva of the woman to rule out anaemia, inspect for signs of
infection, swollen etc.
- From the mouth;
watch the gums and examine the teeth, the colour of the mucosa membrane and
refer if necessary.
- From the neck, watch
for thyroid enlargement. Some enlargement is normal in pregnancy, but if this
is associated with warm, moist hands, tachycardia and a jumpy woman,
thyrotoxicosis should be considered and appropriate tests carried out.
- The breast should
be inspected and palpated to determine the regularity of the breast, lumps and
any flat or inverted nipple.
- Listen to the heart
sound, the rate for any murmurs and carefully check the size of the heart which
might indicate congenital, rheumatic or other disease. Also measure the blood
pressure to rule out PIH.
- Assess the abdomen
for any abnormalities such as enlargement of the liver, kidney or spleen.
- The vagina is
examined for any infection (Candida, gonorrhea, trichomonas, etc.), abnormalities
of the cervix (laceration, erosion etc.), and congenital anomalies such as
double cervix and vagina or vagina septum. Condition predisposing to cervical
incompetence should be carefully evaluated.
- The vulva should be
examined for any varicose, previous tears and episiotomies, state of the perineal
body and laxity of the introitus.
- The limbs are
tested for oedema and the lower limbs for varicosities.
INVESTIGATION CARRIED OUT AT THE
ANC/FIRST VISIT
- Weighing of the
pregnant woman.
- Taking of the blood
pressure to rule out eclampsia.
- Urine test to
confirm pregnancy in certain cases.
- Blood test for Rhesus
factor, haemoglobin, hepatitis B, HIV/AIDS, etc.
- Venereal disease
test such as trichomonas, gonorrhea etc.
- Ultrasound test.
- Urine for diabetes,
ketones, glucose etc.
Danger Signs during
Pregnancy
- Vaginal bleeding
- Reduced fetal
movement
- Frontal or recurring
headaches
- Sudden swelling
- Rupture of the
membranes
- Premature onset of
contraction etc.
High Risk Factors in
Pregnancy
- Domestic Violence.
- Smoking during
pregnancy.
- History of multiple
pregnancy.
- Exposure of mother
to teratogens during pregnancy.
- Presence of maternal
diabetes.
- Previous history of
pre-term delivery.
- History of maternal
hypertension or eclampsia.
- Presence of Sexually
Transmitted Disease.
- Maternal Age.
BASIC PATIENT
TEACHING CONSIDERATIONS FOR THE EXPECTANT MOTHER ON THE FIRST PRENATAL VISIT
WITH REINFORCEMENT ON EACH SUBSEQUENT VISIT
- Instruct the
patient on the importance of regularly scheduled follow-up visits (following
the normal pregnancy).
- Once a month
until the seventh month.
- Every two weeks
during the seventh and eighth month.
- Weekly during
the ninth month until delivery.
- Patient teaching
must continue on each visit.
- Instruct the
patient on the importance of proper nutrition.
- A well-nourished
mother and baby are thought to be far less the victims of obstetric and
prenatal complications, such as:
- Preeclampsia.
- Prematurity.
- Growth
retardation.
- Significant
residual neurologic damage (that is, cerebral palsy, mental deficiency, or
behavior disorders in the child).
2. Guide to good diet
from the six basic food groups daily.
- Milk, yogurt,
and cheese group - 2 to 3 servings per day.
- Meat, poultry, fish,
beans, eggs, and nuts group - 2 to 3 servings per day.
- Vegetable and
fruits - 3 to 5 servings of vegetables and 2 to 4 servings of fruits per day.
- Breads, cereals,
rice and pasta - 6 to 11 servings per day.
3. Proper weight
gain for pregnancy. After an initial loss, the patient will gain 2 to 4 pounds
during the first trimester. Expect a gain of a pound per week during the second
and third trimesters.
 |
| The four basic food groups |
- Instruct the
patient on the importance of proper rest and sleep.
- Pregnancy will
cause the patient to tire more easily.
- Prevention of
fatigue through short rest periods is vital to good health.
- The amount of
rest or sleep required will vary with the individual and stage of her
pregnancy.
- Instruct the
patient on the importance of exercise and fresh air.
- The degree of
exercise will vary according to her condition and stage of pregnancy.
- Walking is usually
the exercise of choice.
- Swimming is an
excellent overall exercise program.
- Instruct the
patient on precautions to take during pregnancy.
- Decrease smoking
or stop altogether if possible.
- Restrict or
limit alcohol intake.
- Avoid children
with measles or other contagious diseases
- Instruct the
patient on potential danger signs of pregnancy that would necessitate her
contacting her physician and visiting a health facility.
- Any vaginal
bleeding, regardless of how small, may indicate miscarriage or abortion,
placenta previa, or placenta abruption.
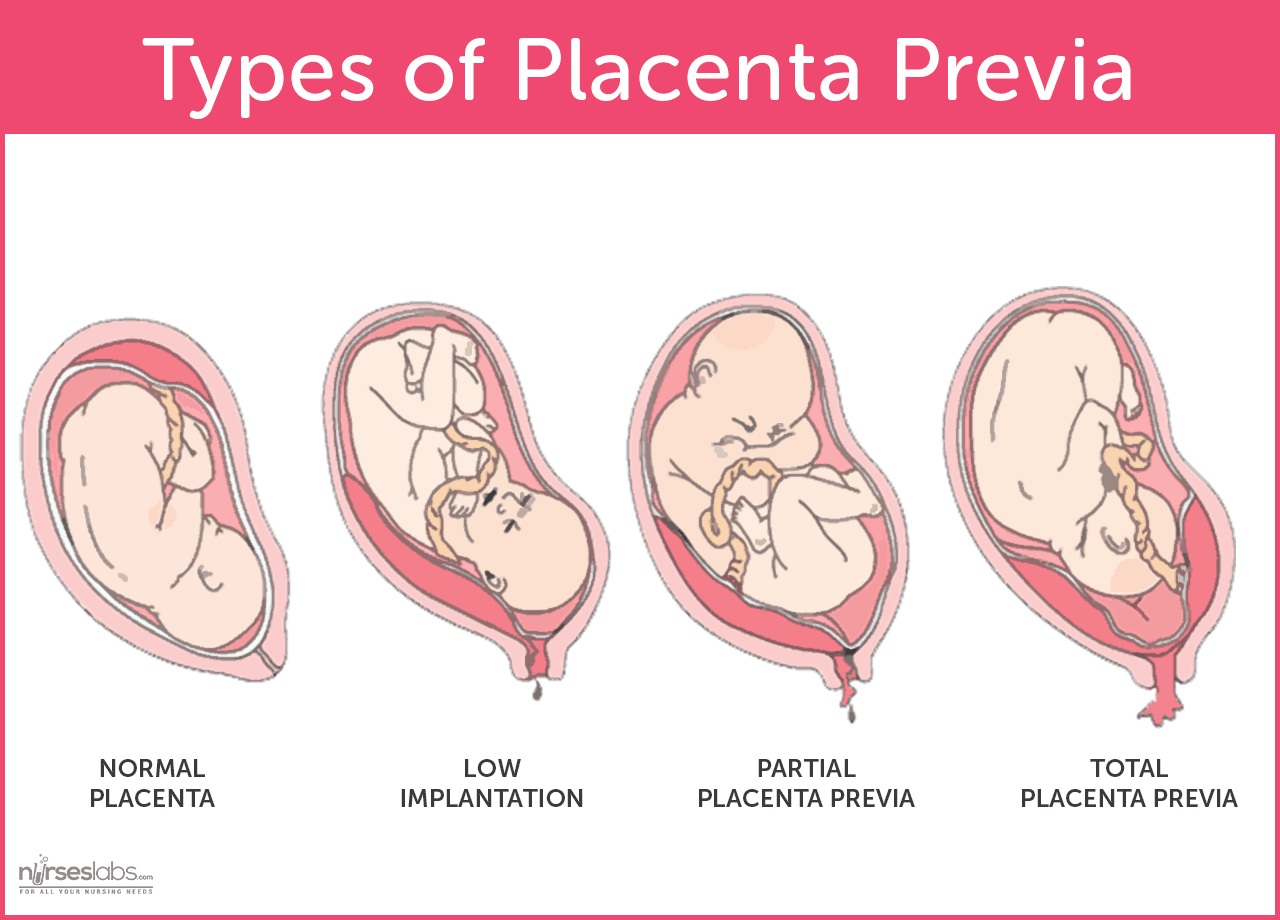 |
Various
degrees of placenta previa. Photo by Nurseslabs
|
 |
| Various
degrees of placenta abruption. Photo by SEIF & ASSOCIATES |
|
2. Symptoms that
may indicate pre-eclampsia. The symptoms are:
- Severe
continuous headache.
- Dimness or
blurring of vision.
- Swelling of the
face or hands, especially when present after resting all night.
- Scotoma - lashes
of lights or dots before the eyes.
- Persistent
vomiting.
- Sharp pain in
the abdomen.
- Epigastric pain.
- Weight gain
greater than 4 pounds in one week.
- Chills and
fever.
- Burning upon
urination.
- Sudden escape of
fluid from the vagina. The patient should report immediately to the physician
or the hospital. She should not wait for uterine contractions to start.
- Lack of fetal
movement over a 24-hour period once "quickening" has been
established.
- Regular uterine
contractions less than 5 minutes apart for an hour for anyone less than 37
weeks pregnancy.
Read Also


Comments
Post a Comment