The fetal circulation
At birth, there is a dramatic alteration in this situation and almost instaneous change must occur. Besides this all, the postnatal structures must be in place and ready to take over.
There are several temporary structures in addition to the placenta itself and the umbilical cord and these enable the fetal circulation to take place while allowing for the changes at birth.
The Umbilical Vein
Leads from the umbilical cord to the underside of the liver and carries blood rich oxygen and nutrients. It has a branch which joins the portal vein and supplies the liver.
The Ductus Vensous
(from a vein to a vein) connects the umbilical vein to the inferior venacava. At this point, the blood mixes with deoxygenated blood returning from the lower parts of the body. Thus the blood throughout the body is a best partially oxygenated.
The Foramen Oval
(Oval Opening) is a temporary opening between the atria which allows the majority of blood entering from the inferior venacava to pass across into the left atrium. The reason for the diversion is that the blood does not need to pass through the lungs since it is already oxygenated.
The ductus arteriosus
(from an artery to an artery) leads from the bifurcation of the pulmonary artery to the descending aorta, entering it just beyond the point where the subclanian and carotid arteries leave.
The hypogastric arteries branch off from the internal iliac arteries and become umbilical arteries when they enter the umbilical cord. They return blood to the placenta. This is the only vessel in the fetus which carries unmixed blood.
Adaptation to extra Uterine life
At birth, the baby takes a breath and blood is drawn to the lungs through the pulmonary arteries. It is then collected and returned to the left atrium via the pulmonary vein resulting in a sudden inflow of blood. The placental circulation ceases soon after birth and so less blood returns to the right side of the heart. In this way, the pressure in the left side of the heart is greater while that of the right side of the heart becomes less. This results in the closure of a flop over the formaen ovale which separated the two sides of the heart and stops the blood flowing from right to left. The cessation of the placenta circulation results in the collapse of the umbilical vein, the ductus venosus and the hypogastric arties. These vessels after collapse change to the following sructures.
The Umbilical Vein becomes the Ligamentaum teres
The Ductus Venosus becomes the Ligamentum Venosum
The Ductus Arteriosus becomes the Ligamentum Arteriousm
The Foramen Ovale becomes the Fossa Ovalis
The hypogastric arteries becomes the obliterated Hypogastric Arteries
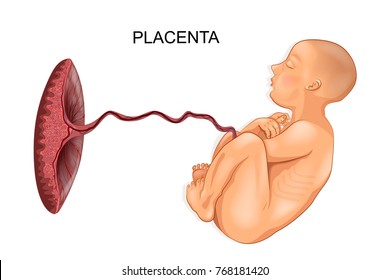
The Placental Circulation
The placenta is completely formed and functioning from 10 weeks after fertilization. Between 12 and 20 weeks gestation, the placenta weighs more than the fetus. Fetal blood, low in oxygen, is pumped by the fetal heart towards the placenta along the umbilical arteries. Having absorbed oxygen the blood is returned to the fetus via the umbilical vein.
The Placenta and Umbilical Cord
DEVELOPMENT OF THE PLACENTA
Its name is derived from a Greek word which means 'cake'. It is purplish red dished shaped mass and looks flat. It develops from chorion and it is continuous with it. At term, it is between 20 and 61.5cm in circumference. It weight about one sixth of the baby birth weight or 500g. It measures about 20cm in diameter and 2.5cm thick in the center thinning out towards the edge.
SURFACE OF THE PLACENTA
It has 2 surfaces
- Maternal surface: it is next to the maternal uterine wall. It is fleshy dark red in color due to the maternal blood in the outer villus spaces. It is covered with thin layer of the decidua and it’s composed of 16-20 lobes (cotyledons) separated by each other by grooves known as the sulci grooves.
- Fetal surface: it is the part towards the foetus in
the uterus. It is smooth, shiny and is covered by the amnion. The foetal blood
vessels can be seen radiating from the insertion of the cord towards the edge
of the placenta.
ABNORMALITIES OF THE PLACENTA
PLACENTA SUCCENTURIATA
this is an accessory lobe attached to the main placenta and blood vessels from the main placenta runs through its membrane and may become retained in utero after the placenta has been expelled.
PLACENTA CIRCUMVALLATA
the membrane on the foetal surface forms a double fold of thick and opaque ring around the edge because of the weakness in its attachment to the placenta.
PLACENTA BIPARTITA OR TRIPATITA
FENESTRATE PLACENTA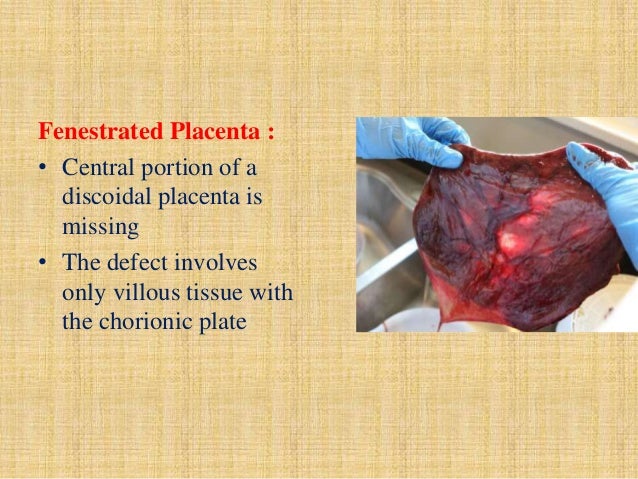
this is the placenta with a window or a hole in it. It occurs when a lobe does not develop and leaves a vacant space.
ABNORMALITIES DUE TO CORD INSERTION
- VELAMENTOUS INSERTION OF THE CORD: the cord is inserted into the membranes away from the edge of the placenta and blood vessels pass through the membrane before reaching the placenta.
- BATTLEDORE INSERTION: the cord is attached right to the placenta with distribution of the blood vessels going towards the centre of the placenta.
DISEASE OF THE PLACENTA
INFARCTS: these are solid white areas of the necrosed (dead) tissue. It is dark in early stages and later appears whitish due to deposition of calcium salts. The size depends on the area affected.
CALCIFICATION OF THE PLACENTA: this is not a real disease, but calcium salts are deposited as nodules on the maternal surface of the placenta at the tips of the anchored villi and the surface of the decidua and the placenta feel gritty.
PLACENTA AGIOMATA OR CHORIO-AGIOMATA: this is a rare condition and is a tumour of the placenta involving the blood vessels. It is a malignant condition.
CAUSES OF PLACENTA ABNORMALITIES
The abnormalities of the placenta are caused by, but not limited to these factors:
- Maternal substance abuse, such as the use of cocaine.
- Ethnicity.
- High blood pressure.
- Multiple gestation pregnancy.
- History of uterine surgery such as a cesarean delivery.
- Maternal blood-clotting disorders.
- History of placental problems.
FUNCTION OF THE PLACENTA
- Respiration: As pulmonary exchange of gases does not take place in the uterus, the fetus must obtain oxygen and excrete carbon dioxide through the placenta.
- Nutrition: Food for the fetus is derived from the mother's diet and has already been broken down into end products by the time it reaches the placenta. The placenta is able to select the nutrients required by the fetus even depleting the mother's own supply in some instances.
- Storage: The placenta metabolizes glucose and can also store it in the form of glycogen and reconvert it to glucose as required. The placenta stores iron and fat soluble vitamins.
- Excretion: The main substance excreted from the fetus is carbon dioxide; bilirubin will also be excreted as red blood cells are released relatively frequently.
- Protection: It provides a limited barrier to infection with the exception of the treponema of syphilis and few other bacteria. Viruses, however, can cross freely and may cause congenital abnormalities as in the case of Rebulla virus and HIV virus.
- Endocrine: Human Chorionic Gonadotropin (HCG) is produced by the cytotrophoblastic layer of the chorinonic villi.
- Oestrogen as the activity of the corpus luteum declines, the placenta takes over the production of estrogen which are secreted in large amount through out pregnancy.
- Human placental lactogen HpL has a role in glucose metabolism in pregnancy.
- Progestrone.
FACTORS THAT AFFECT THE FUNCTION OF THE PLACENTA
- Age of the placenta: from 36weeks of pregnancy the placenta begin to degenerate and if labour does not occurs after 40weeks.
- Maternal disease: in edematous or small placenta, the function is not well performing.
- Development error: in case of infection, tumour and calcification, the placenta does not function well.
- In vellamentous insertion of the cord, the weight of the baby may interfere with the function.
- Partial circulation of the placenta leads to Antepartum Haemorrhage (APH).
- In hemorrhagic disease of the new born, the placenta is too large and edematous.
HOW TO DETECT ABNORMAL FUNCTION OF THE PLACENTA
- A change in the foetal heart rate and volume during auscultation.
- When there is sign of foetal distress.
- It can be detected by the size of the body.
- During examination of the placenta after expulsion from the uterus.
THE UMBILICAL CORD
This is also known as funis. It connects the foetus to the placenta. It extends from the foetal umbilicus to the centre of the placenta. It is about 1.3 - 1.9cm in thickness and average length is 45-50cm. it is dull white colour.
STRUCTURE OF THE UMBILICAL CORD
It is composed of embryonic forms of connective tissue intermingled with gelatinous substance known as Wharton’s jelly. It act as a physical buffer and prevents kinking of the vessels which interfere with circulation. Outwardly, it is covered by a layer of amnion which is continuous from the skin of the baby’s abdomen to the foetal surface of the placenta. It has got 3 blood vessels which are layer and coil in side. The vessels are one umbilical vein and two arteries. The umbilical vein carries oxygenated blood and nutrients from the placenta to the foetus. When the baby needs urgent stimulation drugs can be given into the vein and straight into the circulation. The umbilical arteries are continuation of the hypogastric artery. They carry de-oxygenated blood and waste products from the foetus to the placenta. The artery acts as a protection for the vein.
ABNORMALITIES OF THE UMBILICAL
CORD
- The battledore insertion
- The vellamentous insertion
- The length: it may be short or long.
ABNORMALITIES IN STRUCTURES
There may be 2-4 blood vessels in the cord. This abnormality may indicate absence of a kidney or mongolism.
- False knot: this is a collection of whitish jelly on one side of the cord. It has no ill effect on the foetus.
- True knot: it forms when the foetus turn a lot in the uterus during the first few months of pregnancy. A true knot causes asphyxia and still birth.
Liquor Amnii
The liquor amnii is pale which fills theamniotic cavity and surround the foetus and umbilical cord. It increses and pregnancy advance. It is about 1000mls at term and 800mls remain constant by the wallowing of the fetus. The specific gravity is 1.007 – 1.025 in early pregnancy because it is more concentrated in smaller amount and the PH is neutral to slightly alkaline (7.0 – 7.25). It is alkaline in reaction. It contains albumin, urea, uric acid, creatinine, lecithin sphingomyetin, and bilirubin. It is made of 98.8% of water and 1.2% solid.
Source of Liquor Amnii
It is believed to be the micturition of the fetus.
It is secreted by the cells of the amnion.
It is a translation from the maternal blood and decidua.
It is believed to be made of maternal and fetal vessels.
Functions of the Liquor Amnii
It allows the fetus to grow and move freely.
It prevents adhesion form the fetus to the uterus.
It equalizes the pressure on the fetus in the uterus
It keeps the fetus in an environment to constant temperature.
It protect the fetus from infection so long as it remain intact.
It prevents the full forces of the uterine contraction being exerted on the fetus.
It prevents excessive reduction in size of the size of the placenta size during labour.






0 Comments