CHANGES OF THE SKIN [INTEGUMENTARY
SYSTEM]
Alterations in hormonal balance and
mechanical stretching are responsible for several changes in the integumentary
system. The following changes occur during pregnancy:
- Linea Nigra; This is a dark line
that runs from the umbilicus to the symphysis pubis and may extend as high as
the sternum. It is a hormone-induced pigmentation. After delivery, the line
begins to fade, though it may not ever completely disappear.
- Mask of Pregnancy (Chloasma); This
is the brownish hyper pigmentation of the skin over the face and forehead. It
gives a bronze look, especially in dark-complexioned women. It begins about the
16th week of pregnancy and gradually increases, and then it usually fades after
delivery.
- Striae Gravidarum (Stretch Marks);
This may be due to the action of the adrenocorticosteroids. It reflects a
separation within underlying connective tissue of the skin. This occurs over
areas of maximal stretch – the abdomen, thighs, and breasts. It will usually
fade after delivery although they never completely disappear.
- Sweat Glands; Activity of the sweat
glands throughout the body usually increases which causes the woman to perspire
more profusely during pregnancy.
CHANGES OF BODY TEMPERATURE
- A slight increase in body
temperature in early pregnancy is noted. The temperature returns to normal at
about the 16th week of gestation.
- The patient may feel warmer or
experience "hot flashes" caused by increased hormonal level and basal
metabolic rate.
CHANGES OF THE BREASTS
 |
Changes of the Breast during pregnancy - photo by The Alpha Parent
|
- In early pregnancy, the breast may
feel full or tingle, and increase in size as pregnancy progresses. The areolas
of the nipples darken and the diameter increases. The Montgomery's glands (the
sebaceous glands of the areola) enlarge and tend to protrude. The surface
vessels of the breast may become visible due to increased circulation and turns
to a bluish tint to the breasts.
- By the 16th week (2nd trimester) the
breasts begin to produce colostrum. This is the precursor of breast milk. It is
a thin, watery, yellowish secretion that thickens as pregnancy progresses. It
is extremely high in protein.
- Nursing implication: Inform the
pregnant patient to wear a good, supporting bra.
CHANGES IN BODY WEIGHT
- Normal weight gain is about 24 to 30
pounds (i.e. 10.9 to 13.6kg) during pregnancy.
- Weight gain in pregnancy;
- There is a slight loss of weight
during early pregnancy if the patient experiences much nausea and vomiting.
- She then gains 2 to 4 pounds by the
end of the first trimester.
- A gain of a pound per week is
expected during the second and third trimesters.
- Monitoring of weight gain should be
done in conjunction with close monitoring of blood pressure.
- A lack of significant weight gain
may be an indication of intrauterine growth retardation (IUGR) of the infant.
- Patients with multiple fetuses will
require a higher caloric diet and expect a higher weight gain than a patient
with only one fetus.
- Adequate protein intake should be
emphasized to the patient for development of the healthy fetus and proper diet
reviewed at each prenatal visit.
CHANGES OF THE CIRCULATORY SYSTEM
Blood Volume.
- Blood volume increases gradually by
30 to 50 percent (1500 ml to 3 units). This results in decreased concentration
of red blood cells and hemoglobin. This explains why the need for iron is so
important during pregnancy.
- By the time pregnancy reaches term,
the body has usually compensated for the decrease resulting in an essentially
normal blood count.
- Blood count is interpreted as anemia by
the physician if the hemoglobin falls below 10.5 grams per 100 ml and the
hematocrit drops below 30 percent.
- Increased blood volume compensates
for hypertrophied vascular system of enlarged uterus. It improves the placental
performance. Blood lost during delivery; less than 500 cc (cubic centimeter,
this is the same as ml) is normal (300 to 400 cc is average).
Cardiac Output.
- Cardiac output increases about 30
percent during the first and second trimester to accommodate for hypervolemia.
This is not a problem for patients with a normal heart. A patient with a
diseased heart is especially at risk for cardiac decomposition 28 to 35 weeks
of pregnancy when the blood volume and cardiac load are at their peak; also,
during labor and immediately after delivery when rapid hemodynamic changes occur.
- Change in output is reflected in
the heart rate. It usually increases by 10 beats per minute.
- Nursing implication; Patients with
a diseased heart need to be advised to get plenty of rest and to report any
shortness of breath or unusual symptoms to their physician.
Blood Pressure.
- Normally, the patient's blood
pressure will not rise.
- Nursing implications;
(a) The patient's blood pressure should
be checked carefully and often since a significant increase is one of the
indicators of toxemia (blood poisoning due to toxins) of pregnancy.
(b) When monitoring the blood pressure,
be sure it is done under the same circumstances (that is, patient sitting and
checking from the left arm).
- The lower extremities are often
hampered in the last months of pregnancy due to the expanding uterus
restricting physical movement and interfering with the return of blood flow.
This results in swelling of the feet and legs.
- Nursing implications;
(a) Advise the patient to rest
frequently. This will improve venous return and decrease edema.
(b) Have the patient to elevate her
feet and legs while sitting.
(c) Remind the patient not to lie in a supine position since this inhibits return blood flow as
the heavy uterus presses on the vessels. This leads to the vena cava syndrome
or supine hypotension. The patient may complain of feeling dizzy, nauseated, or
weak
CHANGES OF THE RESPIRATORY SYSTEM
- The respiratory rate rises to 18 to
20 cpm to compensate for increased maternal oxygen consumption, which is needed
for demands of the uterus, the placenta, and the fetus.
- Women may feel out of breath and may
need to sit a moment to catch their breath.
CHANGES OF THE URINARY SYSTEM
- The kidneys must work extra hard
excreting the mother's own waste products plus those of the fetus. There is an
increase in urinary output and a decrease in the specific gravity.
- The patient may develop urine stasis
and pyelonephritis (inflammation of the kidney) in the right kidney. This is due
to pressure on the right ureters resulting from displacement of the uterus
slightly to the right by the sigmoid colon.
- Frequent urination is a complaint
during the first through third trimester. As the uterus rises out of the pelvic
cavity in early pregnancy, pressure on the bladder decreases and frequency
diminishes. When lightening occurs during the final weeks of pregnancy,
pressure on the bladder returns to cause frequent urination.
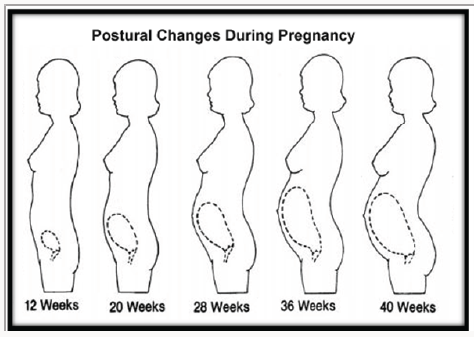
CHANGES OF THE SKELETAL SYSTEM
- There is a realignment of the spinal
curvatures during pregnancy to maintain balance. It is due to the increase in
size of the uterus and pressure on the abdominal wall. The patient walks with
head and shoulders thrust backward and chest protruding outward to compensate.
This gives the patient a "waddling" gait.
- There is a slight relaxation and
increased mobility of the pelvic joints, which allows stretching at the time of
delivery of the infant.
CHANGES OF THE GASTROINTESTINAL SYSTEM
- It was mentioned earlier that as the
pregnancy progresses, the uterus enlarges. It rises up and out of the pelvic
cavity. This action displaces the stomach, intestines, and other adjacent
organs.
- Peristalsis is slowed because of the
production of the progesterone, which decreases tone and mobility of smooth
muscles. This slowing enhances the absorption of nutrients and slows the rate
of secretion of hydrochloric acid and pepsin. Flare-up of peptic ulcers is
uncommon in pregnancy. Slow emptying may increase nausea and heartburn
(pyrosis). Relaxation of the cardiac sphincter may increase regurgitation and
chance for heartburn. Movement through the large intestines
is also slowed due to an increase in water consumption from this area. This
increases the chance for constipation.
- Nursing implications.
(a) If the mother has difficulty with
nausea and/or heartburn, advise her to eat small, frequent meals.
(b) The patient should eat a
well-balanced diet high in protein, iron, and calcium for fetal growth; high
fiber and fluids to prevent constipation.
(c) The mother should not lie flat for
1 to 2 hours after eating because this may cause heartburn and/or
regurgitation.
CHANGES OF SELECTED GLANDS OF THE
ENDOCRINE SYSTEM
- Parathyroid Gland; this gland
increases in size slightly. It meets the increased requirements for calcium
needed for fetal growth.
- Posterior Pituitary; Near the end of
term, the posterior pituitary begins to secrete oxytocin that was produced in
the hypothalamus and stored there. It will serve to initiate labor.
- Anterior Pituitary; At birth, the
anterior pituitary begins to secrete prolactin. This stimulates the production
of breast milk.
- Placenta. The placenta acts as a
temporary endocrine gland during pregnancy. It produces large amounts of
estrogen and progesterone by 10 to 12 weeks of pregnancy. It serves to maintain
the growth of the uterus, helps to control uterine activity, and is responsible
for many of the maternal changes in the body.
Read Also
Management of Normal Labour and Post Natal Care



Comments
Post a Comment